Low Carb High Fat Diet Effect on Cholesterol
Cholesterol and
low-carb diets
- What is cholesterol?
- Cholesterol in your body
- "Normal" cholesterol levels
- Low carb and cholesterol
- Cholesterol increase on low carb
- How to lower cholesterol on low carb
- Advanced testing
- Recommended resources
Cholesterol is an essential component of our bodies and, although there are clear data showing an association between having high blood cholesterol levels and increased cardiovascular risk, it is not clear that cholesterol always equates with increased cardiovascular risk for everyone.1
Read on to learn what cholesterol is, how your body uses it, why low-carb and keto diets may lead to a change in blood cholesterol levels, and whether you should be concerned if your cholesterol increases with a keto or low-carb lifestyle.
The basics: What is cholesterol?
Cholesterol is a waxy substance that is essential for the life of all animals, including humans.2 Cholesterol is found in virtually every cell of your body and is necessary for many bodily functions, including:
- Cell integrity: As an integral part of every cell membrane in the body, cholesterol is required for maintaining cell structure and fluidity.
- Hormone synthesis: Cholesterol is needed to make steroid hormones such as estrogen, testosterone, cortisol, and other related hormones, such as vitamin D3.
- Creation of bile acids: Your liver converts cholesterol into bile acids, which help you absorb fats and the essential fat-soluble vitamins A, D, E and K.
- Myelin formation: The myelin sheath that surrounds and protects nerve cells contains plenty of cholesterol.3
Your body makes most of the cholesterol that is found in your bloodstream. It's primarily produced in the liver.
Dietary cholesterol – found in animal foods like eggs, shellfish, cheese, and organ meat – makes up a smaller portion of your blood cholesterol pool.
Unlike fat, which contains nine calories per gram, cholesterol has no calories. Because it's present in foods in very small amounts, it's measured in milligrams instead of grams. Most fatty meats and whole-milk dairy products contain just a little cholesterol, whereas some shellfish and organ meats are high in cholesterol, yet low in fat.
After years of advice to toss the egg yolks and eat only the whites, we've learned that eating cholesterol-rich foods doesn't impact blood cholesterol levels very much. In fact, when people take in more cholesterol from food, the liver usually produces less, resulting in stable blood cholesterol.4
How is cholesterol transported in your body?
Cholesterol is absorbed from your digestive tract or produced by your liver and circulated throughout your bloodstream, where it can be used by cells as needed. The remaining cholesterol then returns to the liver to be converted into bile acids or used for other purposes.
Importantly, cholesterol doesn't travel around your bloodstream on its own. As a hydrophobic (water-repelling) substance, it must be packaged within lipoproteins to move around the bloodstream.
Think of lipoproteins as boats needed to safely carry cholesterol through the bloodstream. When we talk about blood cholesterol levels, we're referring to the amount of cholesterol contained in different lipoprotein particles (sort of like the number of passengers on the boats).
In addition to cholesterol, these lipoprotein particles also contain special proteins called apolipoproteins, triglycerides, and other compounds.
- Cholesterol packaged in lipoproteins that contain apolipoprotein B100 (usually called Apo B) is referred to as LDL (low-density lipoprotein) cholesterol, or LDL-C (referred to by the more common term LDL for the rest of this guide).5
- Cholesterol packaged in lipoproteins that contain apolipoprotein A is referred to as HDL (high-density lipoprotein) cholesterol, or HDL-C (referred to by the more common term HDL for the rest of this guide).
Despite what we've all heard, there's actually no such thing as "good" or "bad" cholesterol; there is only one type of cholesterol. Your LDL and HDL values refer to how much cholesterol is carried in your HDL and LDL lipoprotein particles. In fact, the same cholesterol is continuously transferred among these and other types of lipoproteins as they make their way through the bloodstream.
LDL is often referred to as "bad" cholesterol because high levels have been linked to increased heart disease risk. By contrast, HDL is frequently called "good" cholesterol because low levels of HDL have been associated with increased heart risk. In addition, one of HDL's main functions is to carry cholesterol back to the liver to be used as needed or excreted through bile.
However, this is an overly simplistic view of LDL and HDL, and it ignores the fact that LDL likely has important beneficial functions. For instance, studies suggest LDL has a role in immune function and injury response, among other roles.6
In addition, this simplistic thinking assumes all LDL is the same, which we would argue is not be the case.7 This is especially true when we consider metabolic disease and its influence on LDL, as well as the role of oxidized LDL.8
So LDL is not inherently "bad" just as HDL is not inherently "good." But they can play good and bad roles in our bodies, depending on the specific situation.
What are "normal" cholesterol levels?
The recommended targets for cholesterol vary slightly among different countries and health agencies. The US National Institutes of Health website lists the following optimal cholesterol and triglyceride values for people at low risk for heart disease, measured after a fast of 9-12 hours:
- Total cholesterol: < 200 mg/dL (5.2 mmol/L)
- LDL cholesterol: < 100 mg/dL (2.6 mmol/L)
- HDL cholesterol: > 40 mg/dL (1.0 mmol/L) for men, > 50 mg/dL (1.3 mmol/L) for women
- Triglycerides: < 150 mg/dL (1.7 mmol/L)
LDL levels >160 mg/dL (4.1 mmol/L) are considered high, and levels 190 mg/dL (4.9 mmol/L) and above are considered very high.
Many factors can affect your blood cholesterol, including genetics, hormonal changes, injury, and certain health conditions. For instance, people with untreated hypothyroidism often have elevated cholesterol.
A person's diet can also influence cholesterol levels – sometimes significantly.9
Some would argue that since these cut-off points are based on epidemiologic studies, they likely do not apply the same to all individuals regardless of their baseline metabolic health and overall health. For instance, there are data that show people with low LDL levels can have heart attacks and people with high LDL can live long lives.10
The point is that LDL levels should be regarded as one of many variables for evaluating cardiovascular risk, using an individual's metabolic status and other risk factors to adjust that risk assessment up or down.
How does keto or low-carb eating affect your cholesterol?
In some people who follow keto or low-carb diets, blood total cholesterol goes up little, if at all. Some even experience a drop in LDL cholesterol after starting low carb. However, others experience an increase in both LDL and HDL cholesterol levels.11 Or, there is an increase only in HDL cholesterol resulting in an improved LDL/HDL ratio.12
One meta-analysis of randomized trials reported that people eating a low-carb diet, on average, experience a reduction in both total LDL and small LDL particles, as well as an increase in the peak LDL size.13
A rise in cholesterol during keto or low-carb eating may be related to losing weight. Although cholesterol levels often drop during the first 2-3 months of losing large amounts of weight, there can be a later rise in cholesterol that persists until weight stabilizes. Once weight loss ceases, cholesterol levels tend to come back down.14
Therefore, it could make sense to wait until someone's weight has been stable for a few months before assessing cholesterol levels.
For an estimated 5 to 25% of people – whether weight loss occurs or not – LDL cholesterol goes up significantly in response to very-low-carb diets, sometimes by 200% or more. Many of these folks seem to belong to a group that Dave Feldman at Cholesterol Code refers to as lean mass hyper-responders (LMHRs).15 These often healthy people are sometimes shocked to discover that their LDL cholesterol has soared above 200 mg/dL (5.2 mmol/L) after going keto.
We realize that quoting data from a blog does not conform to the highest scientific standard. Unfortunately, the medical literature in this field is lacking, so we've decided to present the data that exists. We recognize that Dave's work has not been held up to the same degree of scientific community scrutiny as the papers published in medical journals.
Feldman's theory about lean mass hyper-responders is based on experiments he's conducted on himself and from data he has gathered from hundreds of other low-carbers doing similar self-experiments.
He states that the higher energy demands, lower body fat stores, and lower glycogen stores in these LMHRs trigger the liver to increase production of lipoprotein particles so that triglycerides (fat) can be transported to cells for use as fuel. Since cholesterol travels along with the triglycerides, blood cholesterol levels might rise as the liver pumps out more lipoproteins to keep up with the body's energy demands.
To date, the lipidology community has not endorsed Dave's theory, or any other theory on hyperresponders for that matter. However, other potential explanations exist.
Another theory is that higher saturated fat intake increases cholesterol absorption while a low insulin state decreases LDL receptor activity. The reduced receptor activity thereby decreases the amount of LDL being pulled out of circulation and excreted through bile. When combined, these factors could significantly increase circulating LDL concentration.16
Cholesterol synthesis and absorption are complex mechanisms that are influenced by nutrition, genes, and other factors. Therefore, it isn't surprising that a minority of low-carb dieters experience significant changes in their blood LDL cholesterol levels, and that may be why the exact mechanism remains elusive.
In general, no major concerning serum-lipid changes occur when consuming a ketogenic diet. Typical findings are stable LDL cholesterol levels, a decrease in triglycerides, and an increased HDL cholesterol.17
Should you be concerned if your cholesterol increases with low-carb eating?
This is an emerging area of research that is currently the focus of a great deal of debate and uncertainty.
Traditional experts in the field of lipids and heart disease view elevated LDL cholesterol with concern because it typically reflects a high concentration of LDL particles (LDL-P) circulating in the bloodstream.
Excessive amounts of LDL particles have been found to be associated with the development of atherosclerosis, the underlying cause of heart disease. In atherosclerosis, LDL particles are known to end up in damaged artery walls, and connected to an inflammatory response. Over time, cholesterol, calcium, white blood cells and other substances accumulate at the site to form a plaque. Many – if not most – heart attacks and strokes are caused when a plaque ruptures and forms a clot that blocks arterial blood flow.
The length of time that arteries are exposed to high levels of LDL particles is believed to play a significant role in the development of atherosclerosis. Smaller LDL particles typically spend more time in the bloodstream than larger particles do, making them easier targets for oxidation and incorporation into plaque.18 Moreover, people who have a lot of small LDL particles tend to have low HDL cholesterol and elevated triglycerides – all of which are markers of insulin resistance and reflect increased cardiovascular disease risk.
Even though small LDL particles may be especially problematic, some large studies have also found an association between high concentrations of large LDL particles and heart disease (although these did not control for metabolic health or insulin resistance).19
Despite these associations between high concentrations of LDL particles and heart disease, research has consistently shown that keto diets help reduce many heart disease risk factors in people with diabetes and other insulin-resistant conditions.20 Granted, these are not outcome trials, showing an actual reduction in heart attacks, but those trials don't yet exist. But the demonstrated improvement in risk factors suggests that we may eventually see such beneficial results.
For example, a 2009 randomized study comparing a low-fat diet to a very-low-carb diet in people with metabolic syndrome found that the very-low-carb diet was more effective at improving many cardiovascular health markers, including the following:21
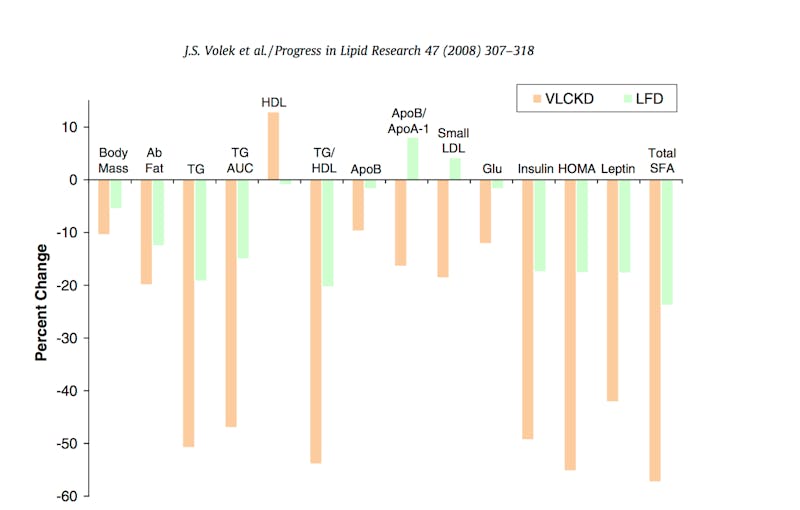
- Decrease in body fat and abdominal fat
- Decrease in triglycerides
- Increase in HDL cholesterol
- Decrease in small LDL particles
- Lower blood glucose levels
- Lower insulin levels
- Increase in insulin sensitivity
Similarly, a nonrandomized trial showed a ketogenic diet reduced the percentage of smaller LDL and increased the larger LDL. This trial also showed no significant increase in atherosclerosis or lipid accumulation in the carotid artery at two-years, even in the hyperresponders.22
The fact that so many risk factors remain stable or improve with carb restriction – even if LDL cholesterol levels increase – demonstrates the importance of not viewing any one value in isolation. Instead, it may be better to look at the body as a whole system.
Prominent lipidologist and vocal lipid educator Dr. Thomas Dayspring, however, urges caution. In his paper "Lipidaholics Anonymous Case 291: Can losing weight worsen lipids?" he states:
"The advocates of low-carb diets say there is no study showing harm of elevated LDL-P and LDL-C in patients who have eliminated or drastically reduced their insulin resistance and inflammatory markers by low carbing. That is true, but what they want to ignore is that there is no data anywhere that shows they are an exception."
Many low-carb proponents, however, counter that none of the studies showing a connection between elevated LDL and heart disease were conducted in people eating keto or low-carb diets.
Dave Feldman is trying to gather as much data as possible about people who have had this experience, and over time, it may very well provide valuable information. If you are a hyper-responder and would like to be part of his ongoing data collection, please get in touch with him by commenting on one of his posts at www.cholesterolcode.com.
At this time, because there aren't any formal studies that have looked at this response, we don't have the ability to predict what will happen long term with people who get very high LDL cholesterol on a low-carb diet.
Five ways to lower your LDL on a keto or low-carb lifestyle
Has your cholesterol increased on a low-carb diet? Do you fear that you may need to abandon this way of eating and its potential benefits?
Here are five ways you can reduce your total and LDL cholesterol levels while maintaining a keto or low-carb lifestyle. Consider trying them in this order.
1. Avoid Bulletproof coffee
Bulletproof coffee refers to adding butter, coconut fat or MCT oil in coffee. Avoid drinking significant amounts of fat at all when you're not hungry. This alone can sometimes normalize elevated cholesterol levels.23
2. Eat only when hungry
Only eat when hungry and consider adding intermittent fasting. This may reduce cholesterol levels. Although most research on intermittent fasting and LDL reduction come from low-quality observational studies during Ramadan, a recent pilot study of time restricted eating showed a significant reduction in LDL.24 While we need more data, this remains a promising intervention.
3. Eat foods higher in unsaturated fats instead of saturated fats
Foods higher in unsaturated fats include fats like olive oil, fatty fish and avocados. Replacing sources of saturated fat with these foods may be enough to lower LDL cholesterol.
However, remember that many unsaturated oils are highly processed. As with food, we recommend focusing on the least processed oils like olive oil, macadamia oil, and avocado oil.
4. Eat LDL-lowering keto-friendly foods
These low-carb plant foods may help lower cholesterol levels somewhat:




- Avocado: An analysis of 10 studies found that eating avocados on a regular basis led to a significant decrease in LDL cholesterol.25
- Green vegetables: Dark leafy greens and cruciferous vegetables bind to bile acids, which are excreted as waste rather than reabsorbed in the gut, ultimately resulting in slightly lower blood cholesterol. To maximize this effect, you may want to steam your greens rather than eating them raw.26
- Cocoa and dark chocolate: In addition to lowering LDL cholesterol, cocoa and dark chocolate might help protect LDL from becoming oxidized or damaged.27 To avoid unnecessary sugar intake, you may want to choose chocolate that contains at least 85% cocoa.
- Nuts and seeds: Nuts and seeds are rich in fiber and monounsaturated fats, which can help lower cholesterol. One analysis of 25 studies found that eating two servings of nuts per day reduced LDL cholesterol by an average of 7%.28
5. Eat more carbs
Finally, if steps 1-4 are not enough: Consider whether you really need to be on a strict keto diet for health reasons.
If a more moderate or liberal low-carb diet (e.g. 50–100 grams of carbs per day) can still work for you, it may also lower your cholesterol. Just remember to choose unprocessed carb sources (e.g., not wheat flour or refined sugar).
Bonus: K2
This is still speculative and no high-quality evidence exists yet. But eating enough foods containing vitamin K2 might help reduce the risk of atherosclerosis.
Vitamin K exists in two forms: K1 and K2. Vitamin K1 is found in plants and is involved in blood clotting. By contrast, vitamin K2 is found mainly in animal products.
There is still no definite proof, but eating enough vitamin K2 might help protect heart health by keeping calcium in your bones and out of your arteries.29The best sources of vitamin K2 include liver, eggs, grass-fed dairy products and chicken.
Advanced testing
As mentioned above, sometimes a rise in LDL cholesterol is temporary, especially during weight loss. However, if yours remains very high and especially if you have additional risk factors (family history of heart disease, certain genetic markers, diabetes, or if you are a smoker), you may want to look into having some advanced testing performed. This may give a clearer indication of your risk profile and state of health, compared to conventional blood cholesterol levels alone:
- NMR spectroscopy (Nuclear Magnetic Resonance): provides detailed information about your LDL and HDL particle sizes and counts, along with an insulin resistance score that reflects your risk of developing diabetes.
- CAC scan (Coronary Artery Calcium): measures calcium accumulation in your coronary arteries by computed tomography in order to identify early signs of heart disease.
- CIMT test (Carotid intima-media thickness): measures the thickness of the inner layer of your carotid artery in order to identify atherosclerosis and lipid deposits.
Recommended viewing and reading
Videos
Dave Feldman: The cholesterol network system
Dr. Andrew Mente: Dietary fat and cardiovascular disease
Sarah Hallberg: LDL on LCHF
Dr. Peter Attia: The straight dope on cholesterol
Articles
Dr. Peter Attia: The straight dope on cholesterol (part 1 of 9)
Dr. Thomas Dayspring: Understanding the entire lipid profile
Cholesterol Code: Are you a lean mass hyper-responder?
Low Carb High Fat Diet Effect on Cholesterol
Source: https://www.dietdoctor.com/low-carb/cholesterol-basics